Many women with desire for abdominoplasty have an umbilical hernia or other hernia associated with large diastases rectus. Provided that these are not complex hernias, they can be repaired safely during the performance of the diastases repair and generally, do not need any supporting mesh as the umbilical hernia repair is reinforced by the correction of the diastases. In this particular case, the patient had an unexpected ventral hernia just above the umbilicus and this was noted during the initial preparation for the diastases repair. Fortunately, Dr. Lyle has had full training in general surgery in preparation for his plastic surgery training and he was very comfortable repairing the hernia having had years of experience. The hernia was repaired directly without mesh and the diastases then repaired. The rest of the abdominoplasty was uneventful, and she had a very nice result. This patient actually was overweight prior to her consultation with a body mass index of 36 that she was able to get her weight down to an acceptable range and therefore Dr. Lyle found her to be a suitable candidate.
Umbilical hernias as well as epigastric hernias frequently occur after weight gain or pregnancies when the thin midline abdominal wall fascia over the structure called the linea alba stretches and weakens. The umbilical remnant is a weak area and is most susceptible to widening creating an opening through which abdominal contents may protrude. The danger of this is that intestinal contents may get entrapped and compromised leading to bowel obstruction and peritonitis. Fortunately, umbilical hernia associated with pregnancy and weight gain primarily have preperitoneal fat present rather than intestine and are unlikely to cause major problems. Umbilical hernia repair during abdominoplasty is not straightforward as special care must be paid to avoid compromising the blood supply to the umbilical skin. In some cases, this is unavoidable, and the umbilical skin can die resulting in a lost umbilicus which would require creation of a new umbilicus.
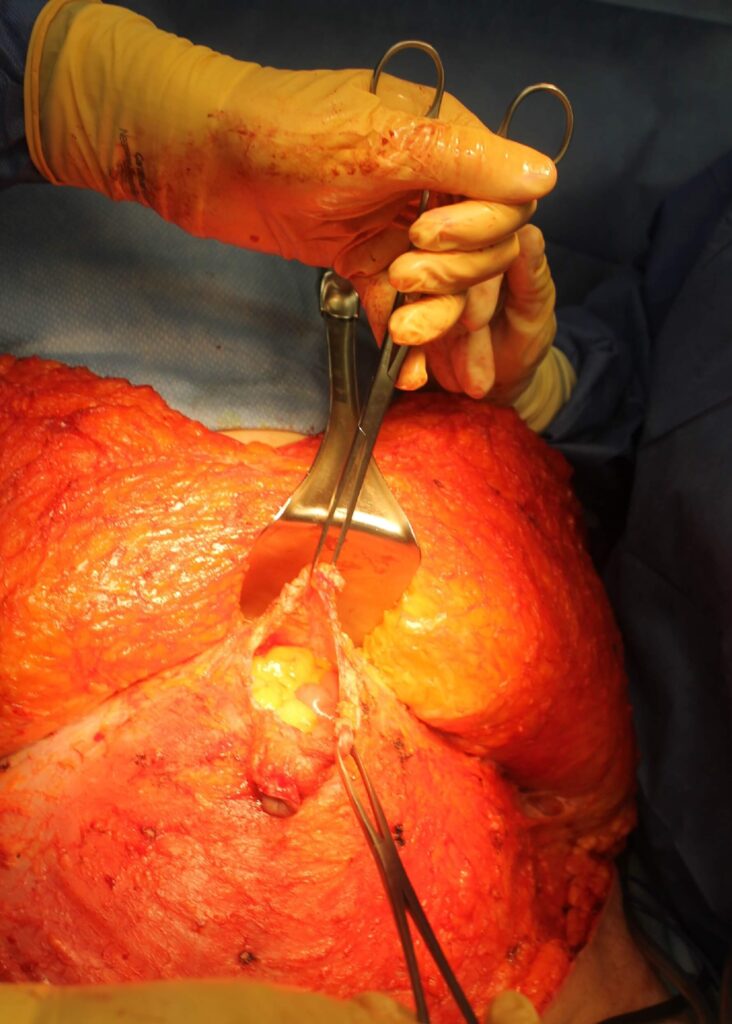
This patient actually had an epigastric hernia above the umbilicus and associated with a previous laparoscopic incision. It was not evident in the preoperative physical exam because her diastases were so prominent. The advantage of having full training in general surgery as Dr. Lyle does, is that these repairs can be managed intraoperatively when they arise unexpectedly.


Further Reading
- Read more about Tummy Tuck Surgery (Abdominoplasty) in Raleigh, NC
- Read more about After Weight Loss Surgery in Raleigh, NC
- Read more Dr Glenn Lyle’s Blog Page on Abdominoplasty with Prior Complicated Umbilical Hernia Repair in Raleigh NC
- Read more Dr Glenn Lyle’s Blog Page on What is a Reverse Tummy Tuck and Who Needs One?
- Read more Dr Glenn Lyle’s Blog Page on What is the Ideal BMI for Tummy Tuck Surgery?

